The Hip Surgery Conversation You Need to Have
Your hip hurts. Like, really hurts. You've tried physiotherapy, injections, medications. Nothing's working. Your doctor says it's time to consider surgery.
Then comes the question: total hip replacement or hip resurfacing?
Most people have no idea there's even a choice. So let's break down what each option actually means, who they're right for, and how to have an intelligent conversation with your surgeon about which path makes sense for you.
Total Hip Replacement: The Tried and True Option
Think of total hip replacement like renovating your entire kitchen. Out with the old, in with the new.
What Actually Happens
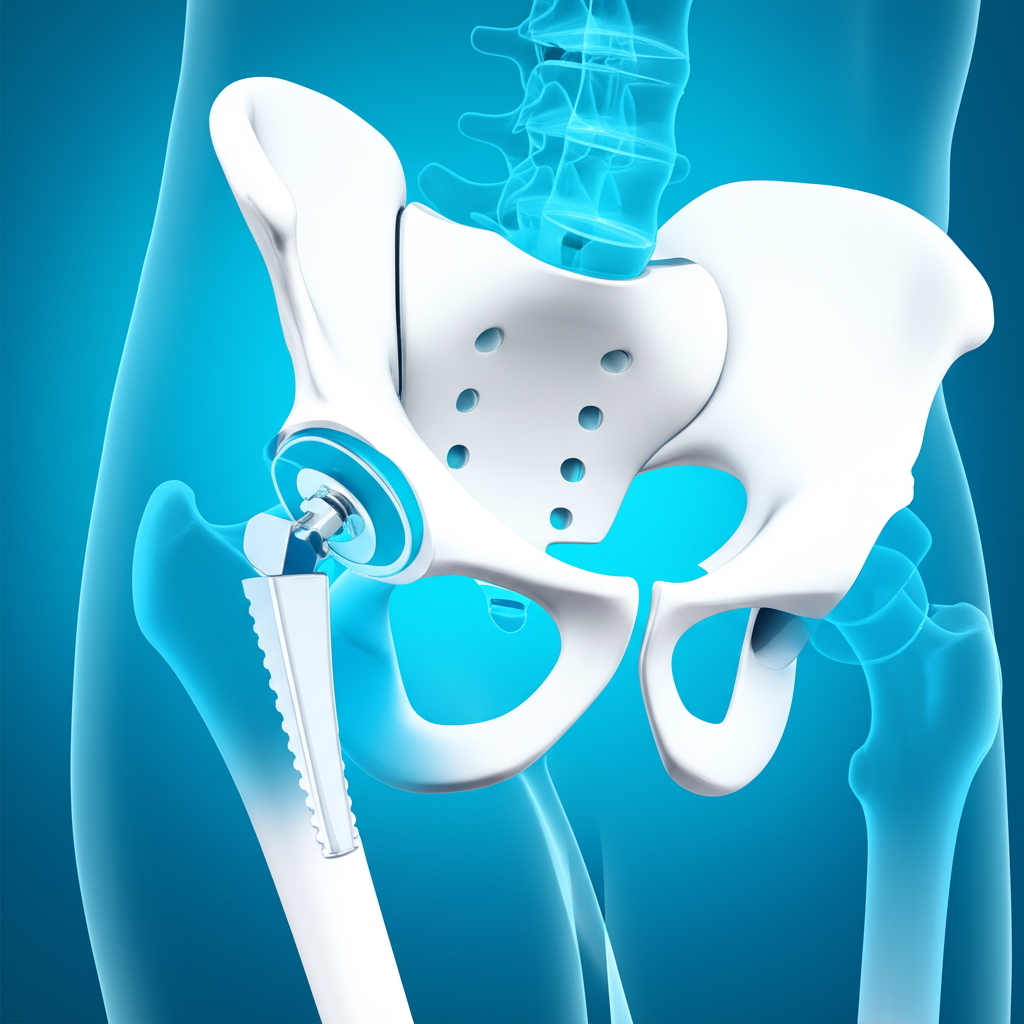
Your surgeon removes the damaged ball at the top of your femur (thighbone) and replaces it with a metal or ceramic ball attached to a stem that goes down into your femur. The damaged socket (acetabulum) gets replaced with a metal cup, usually lined with plastic, ceramic, or metal.
It's been around for decades. Millions have been done worldwide. It works.
Why People Choose Total Hip Replacement
The track record is incredible. Over 95% of people are satisfied with their results. Modern implants last 20-25+ years, sometimes longer. Your grandmother probably had one, and she's probably still walking around just fine.
It works for almost everyone. Elderly patients? Yes. People with bone loss from arthritis? Yes. Those with poor bone quality? Still yes. It's the Swiss Army knife of hip surgeries — versatile and reliable.
The pain relief is dramatic. Most people describe it as life-changing. Activities that were agonizing become manageable. Some even become enjoyable again.
The Downsides Nobody Mentions Upfront
More bone gets removed compared to resurfacing. This matters if you ever need a revision surgery down the road — there's less bone to work with.
There's a small risk (1-2%) of dislocation, especially in the first few months. This is why they give you all those rules about not crossing your legs and being careful getting in and out of cars.
And yes, there's a chance you might need a revision surgery eventually. Implants don't last forever. If you're 50 when you get your hip replaced, there's a decent chance you'll need another surgery in your 70s or 80s.
Hip Resurfacing: The Bone-Conserving Alternative
Hip resurfacing is like refinishing your kitchen cabinets instead of ripping everything out. You're preserving the structure and just putting a new surface on it.
What Makes It Different
Instead of removing the femoral head, your surgeon reshapes it and caps it with a smooth metal covering. The socket still gets a metal cup, similar to total hip replacement. But the key difference? Way less bone is removed.
Why Some People Love Hip Resurfacing
Bone preservation matters. If you're younger and might need revision surgery someday, having more bone left makes that second surgery easier and more likely to succeed.
It feels more natural. Because the anatomy is closer to your original hip, many people report it feels more like their real hip than a total replacement does.
Lower dislocation risk. The ball is bigger, which makes it more stable. You don't have to be as paranoid about hip precautions.
Easier to revise if needed. If the resurfacing eventually fails, converting to a total hip replacement is straightforward because all that bone is still there.
The Catches (Because There Are Always Catches)
Not everyone is a candidate. This is the big one. Hip resurfacing is picky about who it works for.
Metal-on-metal concerns. Some earlier designs had high failure rates and released metal ions into the bloodstream. Modern designs are better, but it's still something to discuss with your surgeon.
Higher risk of femoral neck fracture. The bone under the metal cap can fracture, especially in the first few years.
Requires a highly experienced surgeon. This isn't a surgery every orthopaedic surgeon does regularly. Outcomes are very technique-dependent.
So Who Gets Which Surgery?
You're Probably a Good Candidate for Hip Resurfacing If:
You're younger (under 65). The bone preservation benefits matter more when you have decades ahead of you.
You're male. Sorry, ladies, but the data shows men have significantly better outcomes with resurfacing. It's likely related to bone structure and density.
You're active and want to stay that way. Athletes and people with physically demanding jobs often do better with resurfacing.
You have good bone quality. If arthritis hasn't destroyed the femoral head and neck, you're a better candidate.
You have a larger frame. Bigger people generally have bigger femoral heads, which is better for resurfacing.
You're Probably Better Off with Total Hip Replacement If:
You're over 65. The bone preservation advantage matters less, and total hip replacement has proven results in older patients.
You're female. The success rates just aren't as good for women with resurfacing.
You have osteoporosis or weak bones. Resurfacing needs strong bone to work.
Your femoral head is cystic or deformed from arthritis. There might not be enough good bone to resurface.
You have inflammatory arthritis (like rheumatoid arthritis). Total replacement works better for these conditions.
The Head-to-Head Comparison
| What Matters | Hip Replacement | Hip Resurfacing |
|---|---|---|
| Bone removed | More | Less |
| Dislocation risk | 1-2% | Less than 1% |
| Best age range | Any age | Under 65 |
| Activity level after | Moderate | High |
| How long it lasts | 20-25 years | 15-20 years |
| If revision needed | Standard procedure | Easier to revise |
Recovery: Is One Easier Than the Other?
Honestly? The recoveries are pretty similar. Both involve:
- 2-3 days in hospital
- Walking with aids for several weeks
- Driving again in 4-6 weeks
- Back to desk work in 6-12 weeks
- Full recovery in 3-6 months
Some people with resurfacing feel they recover slightly faster or return to high-level activities sooner, but the research on this is mixed. Don't choose based on recovery timeline — they're close enough that it shouldn't be the deciding factor.
Having the Conversation with Your Surgeon
Come prepared with questions. Here's what actually matters:
"Am I a good candidate for resurfacing based on my specific anatomy?" This requires imaging and a physical exam. There's no generic answer.
"How many of each procedure have you done?" Experience matters enormously with resurfacing. If they've only done a handful, think carefully.
"What are the risks for me specifically?" Your age, gender, bone quality, and activity level change the risk-benefit calculation.
"What activities can I realistically return to with each option?" Get specific. If you want to play tennis or go hiking, ask directly.
"What happens if I need revision surgery down the road?" Understanding the long-term plan matters.
The Truth Nobody Tells You Upfront
Both surgeries can give you excellent pain relief and dramatically improve your quality of life. The difference between them often matters less than choosing a highly experienced surgeon and committing to rehabilitation.
For many people, especially those over 60, total hip replacement is the clear choice. It's proven, reliable, and works for almost everyone.
For younger, active patients with good bone quality — particularly men — resurfacing might be worth considering. But only if you have a surgeon with extensive experience in the procedure.
The "best" choice depends on your age, activity level, anatomy, and personal goals. This isn't a one-size-fits-all decision.
Make the Choice That's Right for Your Life
Talk to your surgeon. Understand your options. Ask questions until you feel confident you understand the trade-offs.
Whichever path you choose, the goal is the same: getting you back to living your life without hip pain. And both surgeries can absolutely do that.